phre·nol·o·gy/frəˈnäləjē/ the detailed study of the shape and size of the cranium as a supposed indication of character and mental abilities.
The article YOUR DOPPELGÄNGER IS OUT THERE AND YOU PROBABLY SHARE DNA WITH THEM in today’s The New York Times was surprising and not surprising at the same time. I grew up reading old medical books and (often racist) cartoon collections from the tail end of the heyday of phrenology in the 1940s. Nobody around me really believed in it, and the idea that our looks are linked to our character doesn’t seem to fit with the ideas of no discrimination and equal opportunity.
But here we are: The NYT article reports on a large study of doppelgängers, people who look like twins without being related in any way. Such couples share more DNA than random pairings. And what is even more interesting is that the degree of similarity in their personalities is more closely linked to the amount of shared DNA than to the similarities of their life experiences.

The article even hints that this research could lead to forensic use, such as predicting the facial features of a suspect just from crime scene DNA samples.
Dr. Esteller also suggested that there could be links between facial features and behavioral patterns, and that the study’s findings might one day aid forensic science by providing a glimpse of the faces of criminal suspects known only from DNA samples. However, Daphne Martschenko, a postdoctoral researcher at the Stanford Center for Biomedical Ethics who was not involved with the study, urged caution in applying its findings to forensics.
How far are we then from again linking facial features to moral character?
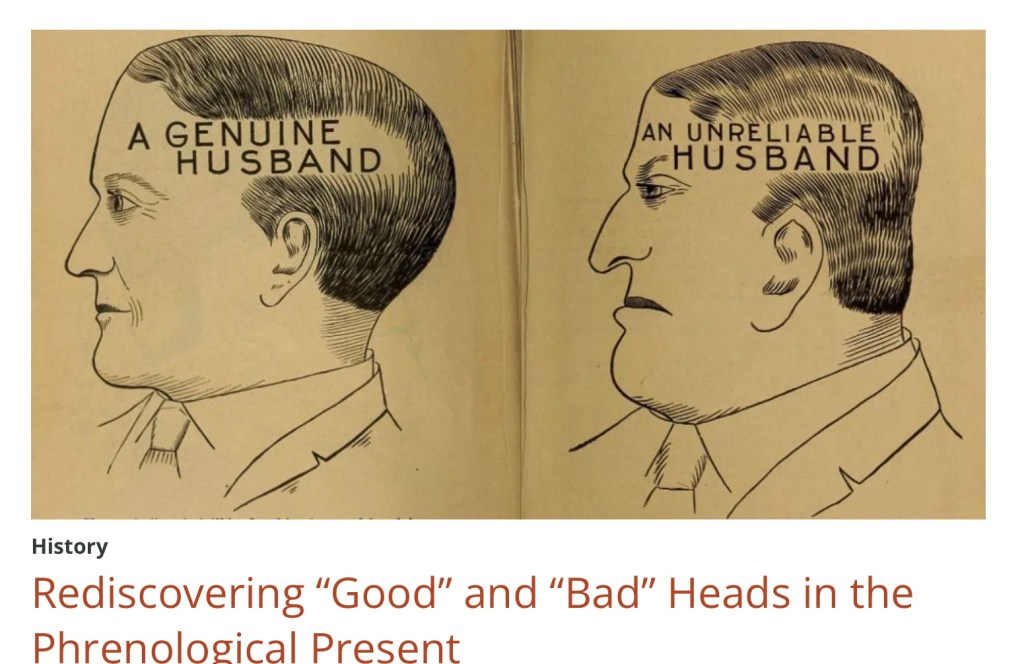
“While on the one hand I was pleased to see so many commentators connecting the conclusions of this study to phrenology, physiognomy, and related sciences, this leads to its own problems. Most modern-day commentators (and many historians) continue to frame phrenology primarily as a “pseudo-science,” a term often used to dismiss “bad” science. But in so doing, they neglect the long-term influence of phrenology and related “failed” sciences. By dismissing this study as yet another example of phrenology, without simultaneously recognizing the historic scientific validity, utility, and pervasive nature of the science, commentators highlight its superficial aspects while enabling the continued influence of the underlying principles. This study demonstrates the continued influence of phrenological thinking, language, and imagery in modern culture – both popular and scientific.”












{kind=link}