I Learned a New Word Today: RECRUDESCENCE – NEJM
The New England Journal of Medicine’s question of the week was about an elderly man with a prior stroke history, who during a febrile illness had a temporary recurrence of his original stroke symptoms.
“Patients who have had neurologic deficits as a result of stroke or multiple sclerosis sometimes experience reemergence or recrudescence of those deficits in the setting of an intercurrent illness. The most common triggers include infection, hypotension, hyponatremia, hypoglycemia, insomnia, stress, and benzodiazepine use. Recrudescence occurs most commonly with middle cerebral-artery infarcts and can lead to language, sensory, and motor deficits. Gaze preference, hemianopsia, and neglect are not typically observed.”
Diabetes Related Hospitalizations Not Necessarily Caused by Poor Outpatient Management – JAMA
Quality is an elusive thing: JAMA Network Open has a piece about what kind of correlation there is between the diabetes quality indicators we all deal with in primary care and what really happens to patients. Any guesses?
In this study, the associations among different types of diabetes quality measures were weak, and much variation in the rates of utilization-based outcomes was unexplained by clinical practice group performance on traditional process and disease control measures. This outcome may be due in part to the topped-out nature of process measures, but the weak association between clinically robust disease control measures and hospitalization rates, the modest difference in hospitalization rates based on process and disease control performance, and the small amount of variation between clinical practice group hospitalization rates explained by process and disease control performance all raise concern about the validity of utilization-based outcomes as a measure of quality in chronic diseases. In chronic diseases such as diabetes, more hospitalizations may not necessarily be evidence of poor outpatient care, which has significant implications for quality-based reimbursement in chronic disease management.
— Read on jamanetwork.com/journals/jamanetworkopen/fullarticle/2747756
Family health history: underused for actionable risk assessment – The Lancet
I’m making a plug again for The Lancet, which has lots of free material, available just by registering.
Here’s something so basic we should be ashamed for not making better use of: The FAMILY HISTORY. Now that there are genetic markers and all, why don’t we pay more attention to obtaining a proper Family History?
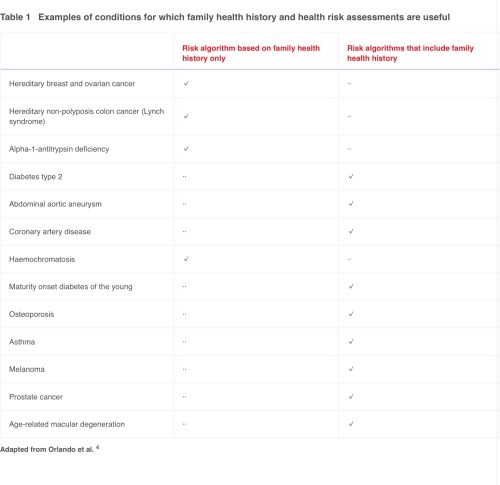
If applied across the general population, systematic FHH-based risk assessment has the potential to have a substantial effect on population health management. Up to 44% of people meet criteria for increased risk for at least one hereditary condition based on current guidelines, so the potential for impact on health is huge.40 Scaled to a population, FHH becomes a means of assessing the true risk and potential costs that a health system might use to better manage its financial risk. When multiplied to potentially affected family members, the effect becomes even greater.
— Read on www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)31275-9/fulltext












{kind=link}
Interestingly, I don’t think my PCP/Family Doc Group has asked about an update on my family history since I started going there in 1999. Since then, my mother died of an MI at age 63, and my father has vascular dementia. Seems to me the family history should be an ongoing thing. I’ll bring it up with my next physical, but shouldn’t it be SOP?
My emrs make you a) click that you have reviewed it and b) manually import it. (Not necessarily update…) You know what the problem is? Too many mandated screenings for a fifteen minute visit. The family history update can be fudged, just by importing/clicking on the old one. The depression and alcohol ones can’t be imported/copied &pasted.