McDonaldization of Chronic Pain Therapy (and All of Primary Care?) in the USA – BMJ
A recent Open-Access piece in the British Medical Journal about what they called the “McDonaldization of Chronic Pain Therapy” made me think that this phenomenon, which I hadn’t heard called that before, was certainly present in Primary Care, too. I have sometimes found myself saying, or at least thinking, that 15 minute medicine is more like McDonald’s than fancy restaurants.
The article lists four dimensions of what they have termed McDonaldization:
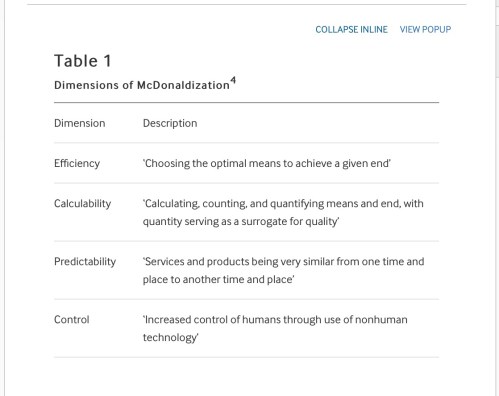
Number four stopped me cold – this is Healthcare today. The BMJ article states:
“The fourth dimension of McDonaldization is control—control of employees, of the system and of consumers. McDonald’s uses a controlled system, comprising a combination of humans, computers and cooking technologies to serve ‘precut and preprepared food’ to hungry customers, eager for their salty fix. This system minimises the need for human creativity and effort on the part of both employee and consumer. In the context of chronic pain management, OxyContin worked very similarly and thus produced a strange control over both doctor and patient. Physicians no longer had to parse out what exactly the cause(s) of a patient’s pain was and what therapies they might benefit from, but rather, now had the option of giving one drug to keep it all at bay.
Purdue Pharma’s aggressive and patently false advertising of the safety of the drug positioned OxyContin as the most rational and efficient choice a physician could make in treating a patient in pain. This only served to benefit the controlled McDonaldized system Purdue Pharma was helping construct, because people—physicians included—are ‘the great source of uncertainty, unpredictability and inefficiency in any rationalizing system’.
The responsibility of treating patients with chronic pain often falls to primary care physicians, and as such, they were Purdue Pharma’s prime target in expanding the ‘OxyContin prescribing base’. With the increasing demands of medical McDonaldization, one of the highest burnout rates of all physician specialties, and the shortage of primary care physicians ever growing, they were understandably susceptible to believing the promises of the drug. Furthermore, these physicians were already fighting multiple American epidemics, like pre-diabetes and hypertension (for which McDonald’s itself happens to be a significant contributor). So, if there was a quick, effective treatment for another complex finding—pain—available, then there was little desire or opportunity to take the time to question the legitimacy of Purdue’s claims. Thus, they prescribed the drugs liberally, as they were instructed to at their Purdue-funded educational conferences.”
Yours truly wrote a little while ago about the downside of even using the word “treatment” for chronic conditions, instead thinking “guidance” better describes what we ought to be providing.
“Treatment”, the second part of the traditional duad, is too simplistic a notion, only useful for lancing boils and prescribing penicillin for strep throat. Most diseases are multifaceted and most patients have several health and disease considerations. Most diseases are also chronic, even ones we thought of as rapidly terminal earlier in our own lifetime, like HIV and an increasing number of cancers.
The physician’s role is not a knee jerk intervention, it is informing and educating the patient and helping each patient choose a plan of action that is right for them.
Primary Care does what Google can’t, it applies knowledge of the patient and of the relative importance of medical facts and factoids and offers guidance in the sense of ranking options.
https://fmch.bmj.com/content/7/1/e000069
Does Anybody REALLY Want to Fix Physician Burnout?
In my inbox the other day was an AMA update that was mostly about burnout:
http://www.massmed.org/News-and-Publications/MMS-News-Releases/Physician-Burnout-Report-2018/
This is getting out of hand. We have two crises converging to soon cripple and bankrupt our health care system and quite possibly our entire economy:
1) An aging population and people of all ages that are increasingly affected by chronic diseases that were rare a generation ago.
2) A burned-out, disillusioned and hamstrung medical profession, unable to do anything in their allotted 15 minute visits about the lifestyle-dependent epidemics beyond prescribing $400-$1,000 a month drugs that allow the disease snowball to keep rolling and growing, albeit at a somewhat slower rate.
I recently wrote about burnout:
“Put simply: If anybody wants to define and manage our work for us instead of letting us do it, they become responsible for the outcomes if we aren’t given the time or the tools we, as the ones who went to school, know we need.
The cure for physician burnout is simple: Listen to us when we say what we need in order to do our best. We didn’t spend all this time and energy so we could collect our salaries and goof off.
Most of us still have a professional mindset. We want to do a good job and we know how to do it. Let us.”
BUT, as one commenter wrote:
“Well said, and so true. But the solution is NOT ‘simple”, because THEY will never listen to us. The difficult, but only realistic solution is to be independent…”
So, we need some honest answers and some new paradigms here:
What is disease?
What is public health?
What do we need doctors to do if there are so few of them?
Does every “stakeholder” benefit if people get healthier? Or do some profit from continuing worsening of our nation’s health?
That last point is obviously rhetorical. What kind of health care system can reconcile when insurance companies and pharmaceutical companies actually profit from people being sicker?












{kind=link}
0 Responses to “A Country Doctor Reads: February 2, 2019”