An overweight man with high blood pressure asked me about Ozempic the other day. He and his wife have different insurances. She is on Ozempic with a low co-pay. It would be high enough to be difficult for my male patient to afford.
So I asked him: “What does it feel like to be hungry?”
“I don’t know”, he answered. “I can work all day without even eating breakfast and feel fine but then once I start eating, I just go on and on. I’m not much of a snacker, I just eat big meals.”
“I have a large hiatal hernia with spontaneous reflux even standing up”, I started. “If I go too long between meals, I get acid reflux and pain in my upper belly. And sometimes I get cranky and confused”, I explained.
“I don’t feel any of those things”, he said.
My response was instant like a divine flash of lightning from the sky: “Why don’t you let your wife plate your food, just the size portion that she is eating?”
He smiled and raised his eyebrows.
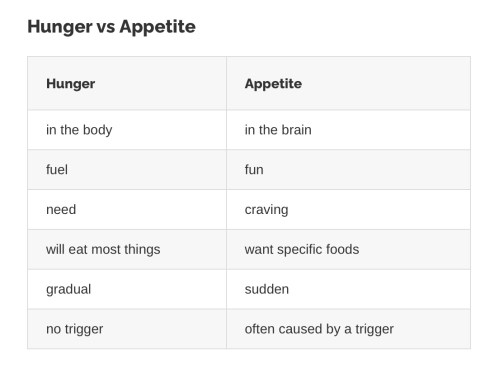
“Because you don’t feel hungry, you just have an appetite. Doing this would save you a lot of money and avoid piling more medication on top of what you’re already taking. It might be worth a try”, I said.
“Let your wife be your Ozempic”, I added. “And if you haven’t lost any weight when you come back to see what this new blood pressure pill is doing for you, we can talk Ozempic and other options if you’re still interested!”
https://badgut.org/information-centre/a-z-digestive-topics/hunger-and-appetite/












{kind=link}