Many physicians have become world famous writers and in Greek mythology, Apollo was the god of both poetry and medicine.
I can personally think of many prominent physician writers I have come across in my reading over the years:
There was the 12th century rabbi Maimonides, Copernicus in the 15th century and the poet John Keats in the 1700’s.
In the late 1800’s to early 1900’s there were Anton Chekhov, Sir Arthur Conan Doyle and William Somerset Maugham.
Examples from our time (or at least mine) are A J Cronin (Dr Finlay) Robin Cook (Coma), Viktor Frankl (Man’s search for meaning), Michael Chrichton (Jurassic Park), the Polish science fiction writer Stanislav Lem, M Scott Peck (The Road less traveled), Oliver Sacks, Frank Slaughter, Sherwin Nuland, Walker Percy and more recently, Mainer Tess Gerritsen.
But you wouldn’t think doctoring and literature are even remotely connected after reading what my colleagues and I are producing every day in our electronic medical records.
In journalism school and writing classes they tell you how to capture the reader’s attention and make your point effectively. They teach how to make the readers feel like they are witnessing real events and experiencing the emotions of the characters of the writing.
In medical charting class, and when using EMRs, the priority is to prominently list the items that are required for payment and compliance purposes.
Evaluation and Management (E&M) reimbursement codes are built around how many aspects of a symptom or a physical exam are documented. Sometimes called “bullets”, each one is usually a separate sentence in the “printout” display of a medical record whereas to the documenting physician they may be a click box. Looking at the computer screen, they are sometimes quick to review, much like the paper forms I used to create for upper respiratory infections, urinary tract infections and physicals etcetera in the days of paper records. But when our computer programs turn these checkboxes into sentences, they look more like “See Spot run” grade-school English than an expert clinician’s narrative.
Here are two screen shots from a clinic a couple of towns north of here:
Writer’s view:
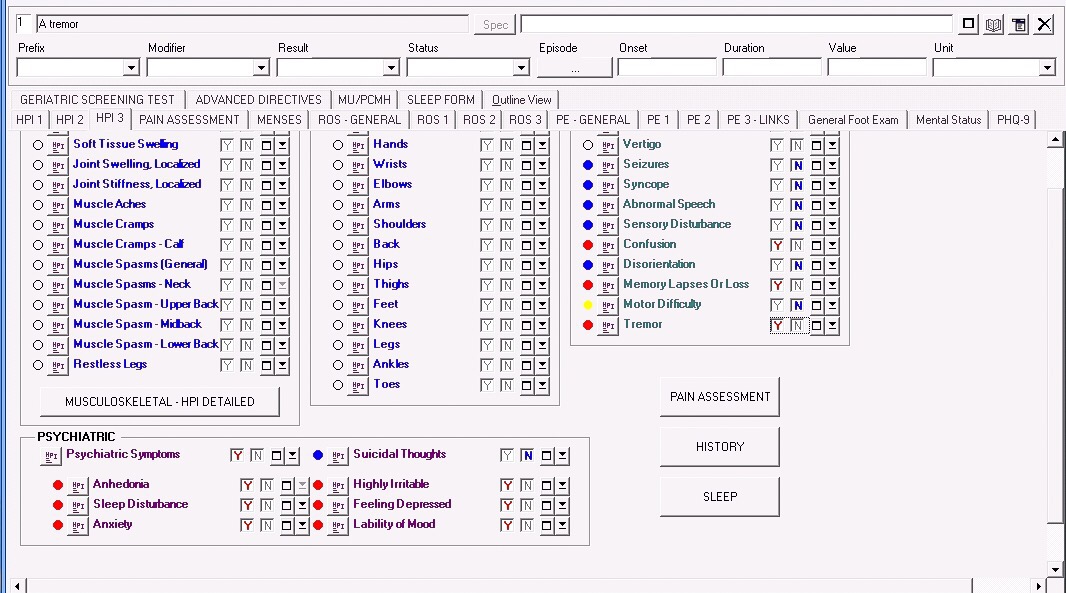
Reader’s view:

Anybody who tries to quickly read such notes would probably just as soon see the original clickboxes, instead of the stilted English produced by the EMR.
Back to the real writers among us – here is how Abraham Verghese explains the deep connection between doctoring and writing:
“I’m really struck by how much of what I learned in medical school has helped me to be a writer, and how much of what I learn as a writer helps my thinking as a physician. They are very parallel disciplines. When you take a patient’s clinical history, what is that but a story? What makes a good doctor is that he or she takes the story down well, sees the links and makes the connections toward a diagnosis. That’s also what writing is about.”
I guess that’s why, after a long day with my patients and my highly structured EMR, I like to sit down in my den next to the horse stalls with a completely blank screen in front of me and just tell stories.













{kind=link}