I pay $500 per year for UpToDate, the online reference that helps me stay current on diagnostic criteria and best treatment options for most diseases I might run into in my practice. They also have a rich library of patient information, which I often print out during office visits.
I don’t get any “credit” for doing that, but I do if I print the, often paltry, patient handouts built into my EMR. That was how the rules governing meaningful use of subsidized computer technology for medical offices were written.
If I describe in great detail in my office note how I motivated a patient to quit smoking but forgot to also check the box that smoking cessation education was provided, I look like a negligent doctor. My expensive EMR can’t extract that information from the text. Google, from my mobile device, can translate between languages and manages to send me ads based on words in my web searches.
When I do a diabetic foot exam, it doesn’t count for my quality metrics if I freetext it; I must use the right boxes. If I do it diligently on my iPad in eClinicalWorks, one of my EMRs, even if I use the clickboxes, it doesn’t carry over to the flowsheet or my report card.
Not only are these things annoying and part of the mounting overall frustrations of being a doctor, or PA/Nurse Practitioner, today. They are also misguided; I may document a foot exam or provide a disease specific handout, but then what?
Our primitive technology can’t automatically do anything more. Did the printed information change my patient’s behavior? Did the foot exam reveal diabetic complications, and did I do anything about that? Did my smoking cessation advice (CPT code 99406) produce results? Or did the patient quit on her own because her sister got lung cancer?
More and more, I am thinking we, as providers, are measured too much for the wrong things.
I also think that, more and more, we are expected to do the wrong things.
My diabetic patient may see a well qualified podiatrist, who spends a great deal of time examining and treating my patient’s feet, but I am the only one who can prescribe the diabetic shoes. How detailed does my foot exam have to be for that prescription to count? Not very, mostly clicking the designated box.
I don’t double check the retina specialist’s work examining and injecting my diabetic patient’s eyes, now, do I? I am only charged with documenting that my diabetic patient sees the eye doctor. I wonder why Medicare needs me to tell hem that when they are presumably paying big money for that to happen?
In our fifteen minute world, wouldn’t it be better if I had time to read the podiatrist and eye doctor reports and use them to help motivate my patient to eat differently and exercise more? Instead of:
Have you seen the eye doctor? Check.
Have you seen the podiatrist? Good, let me check your feet real quick so I can say I did it and get you the shoes he wanted you to have…Check.
And do you know smoking is bad for you? Check.
Do you know too many carb calories raise blood sugars and cause weight gain? Check.
You don’t drink too much, do you? Check.
Not too depressed this time of year? Check.
Did you get your flu shot, colonoscopy and Pap smear? Check.
And what about hepatitis C, domestic violence and making out those Advance Directives? Check.
Makes me feel I’m a great doctor. Or does it?
There is another dimension of Medicine, invisible to those who measure us, but it is the only one our patients see.
 Today, in Van Buren, I called the small local Rexall (a historical U.S. pharmacy name) and chatted with the owner, John Hebert. He has Kayexalate in stock. This is in a town of 2,000 people. From Bangor to Ellsworth to Belfast I imagine there are 100,000 people. They don’t have outpatient access to this drug.
Today, in Van Buren, I called the small local Rexall (a historical U.S. pharmacy name) and chatted with the owner, John Hebert. He has Kayexalate in stock. This is in a town of 2,000 people. From Bangor to Ellsworth to Belfast I imagine there are 100,000 people. They don’t have outpatient access to this drug.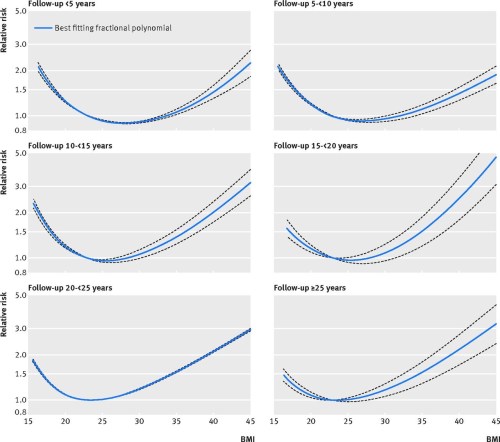 It is sobering to look at the exponential increase in death risk when BMI exceeds ideal: 20% excess risk for even average Americans, 50% greater risk at a BMI of 35 and double the risk at a BMI of 40.
It is sobering to look at the exponential increase in death risk when BMI exceeds ideal: 20% excess risk for even average Americans, 50% greater risk at a BMI of 35 and double the risk at a BMI of 40.











{kind=link}