Why is depression now the leading cause of disability worldwide? I have been thinking and reading about this more and more, and the theories are many, from genetics to what we ingest to general stress to smartphones.
It has all seemed a bit vague – until I came across the concept of Perceived Social Support (PSS) score. It is a way to consolidate and quantify all the effects our modern life seems to have on our mental health by looking inside ourselves before considering the nature of the external forces, which may differ from one person to another.
The Oslo Social Support Scale, perhaps the most concise rating scale, is a simple scoring system based on three questions. It was first used in research to make comparisons between recent immigrants and people born in Norway. Not surprisingly, a poor OSSS score was a predictor of poor mental health.
► Oslo 1: How many people are you so close to that you can count on them if you have great personal problems? (none (1), 1–2 (2), 3–5 (3), 5+ (4))
► Oslo 2: How much interest and concern do people show in what you do? (a lot (5), some (4), uncertain (3), little (2), none (1))
► Oslo 3: How easy is it to get practical help from neighbours if you should need it? (very easy (5), easy (4), possible (3), difficult (2), very difficult (1))
More recently, this simple scoring system has been used to quantify the risk that Adverse Childhood Events (ACE) will cause adult depression. A favorable Perceived Social Support score, PSS, (factual or not, our perception is what matters) can act as a buffer, or a resilience factor if you will.
Exposure to ACE was assessed using the ACE questionaire, which addresses 10 individual ACEs under three categories:
► abuse: emotional, physical and sexual abuse
► neglect: emotional and physical neglect
► household dysfunction: parental separation/divorce, violence against mother, household substance abuse, household mental illness and incarceration of household member.
A low PSS score may increase the risk of depression five-fold for people with a history of three or more Adverse Childhood Events according to a 2017 paper in the British Medical Journal:
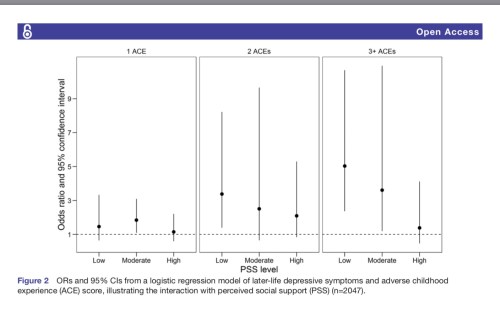
(https://bmjopen.bmj.com/content/bmjopen/7/9/e013228.full.pdf)
Perceived Social Support is like a prism through which we interpret external factors, or like sets of filters for photographic effects – sepia, cold, warm or black and white.
The obvious conclusion to be drawn from the link between Perceived Social Support and mental health, drawn by many but perhaps not always so neatly explained and quantified, is to look at all the circles we belong to or may be able to join and see how we can contribute to those micro communities.
Because, and this is the magic of understanding PSS, when you offer yourself as a support or resource to others, you usually get multiples of your input in return from those you help.
As I finish writing this reflection, which I started outlining last month, the inevitable and obvious context becomes “Who will have the most severe mental health symptoms develop as a consequence of natural disasters and pandemics?” I think the PSS score is a good predictor here, too.
And, as I am right now in self quarantine while waiting for the results of my COVID-19 test, the obvious question isn’t how much Social Support I objectively have, but whether I feel I have enough.













{kind=link}