A few weeks ago, I saw a patient with shortness of breath during my Saturday clinic. He had been short of breath for a few of weeks, and on a couple of occasions he had also experienced mild chest pain. He has known aortic stenosis, moderate according to his last echocardiogram two years ago.
My brain kicked into autopilot and I asked “have you fainted or passed out recently?” It was a flashback to medical school, where it seemed we were inundated with lists of threes.
For aortic stenosis, the triad of surgical indications for critical degrees was: Angina, synkope (remember I’m Swedish) and svikt, which is Swedish for failure, specifically congestive heart failure.
I’ve already written about a diagnosis right under my nose that I missed because the onset was so gradual: Dementia, urinary incontinence and gait disturbance, the diagnostic triad of normal pressure hydrocephalus.
A few months ago a crackerjack nurse practitioner came to me with the question: “What’s the syndrome with a droopy eyelid and a small pupil?”
“And a sunken-in eyeball?” I added.
“Yes!” She exclaimed.
“Horner’s Syndrome”, I proclaimed. “I still remember it from medical school and from a patient and my first Persian cat who both had sinus cancer.”
I don’t know why there are all these diagnostic triads out there, is it by some divine design or just because medical students can only retain short lists because of the multitude of diagnoses we have to memorize?
Where would we be without memorization? Sure, we could use computers to sift through endless lists of symptoms, most of which are red herrings, but there’s nothing quite as satisfying as knowing, in an instant, what the diagnosis is.
Wikipedia has a list of fifty clinical triads:
https://en.m.wikipedia.org/wiki/List_of_medical_triads_and_pentads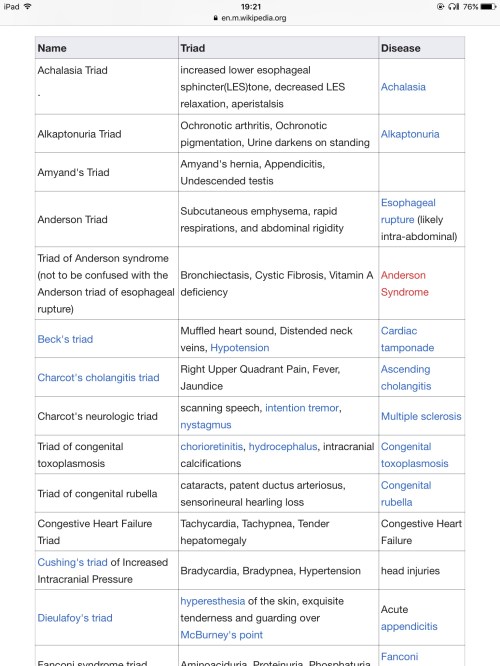
And, I almost forgot, last week I saw a patient with Reiter’s Syndrome, now called Reactive Arthritis: Persistent conjunctivitis, frequent urination and migrating arthritis that all began after a bout of severe diarrhea. She had already seen one other primary care clinician and her optometrist and both knew there was a bigger, overarching diagnosis behind her eye irritation. I was the one who nailed it.












{kind=link}