A clinical encounter from 1980 recalled in a 2010 blog post and just think how far we have come since then.
We certainly live in the knowledge economy, a world where having information and knowing how to use it is the key to success in just about any field.
And there’s so much more of it now. I remember having a book when my children were young titled something like encyclopedia of trivia. Just one thin volume? That’s unfathomable now.
Back in 1980 in one of my first rotations in my Swedish internship, which was a 20 or 21 month affair, I was a prison doctor in a sparsely furnished room with only two books on the bookshelf. One of them was a well read older Merck Manual which helped me make a diagnosis that seemed life-changing to one of the inmates.
I now can check Google AI, Epocrates, Up-to-Date, the National Library of Medicine and countless other websites from my iPhone 13 mini, which fits easily in my left front pant pocket. If I’m looking for the exact name or the exact treatment or the main criteria for any diagnosis, it is literally at my fingertips and it has been for several years so I think I am part of a groundbreaking generation of physicians who went from looking things up in a book to checking them out on my personal iPhone.
It’s a little bit like my grandfather‘s experience with cars, having been the first one in his village to drive one, or my parents experience with charter flights to the Mediterranean. Once exotic, later commonplace inventions changed the world in less than a generation in the last 100 years.
Im quirky in several ways. One is that I have an aversion to drinking water. It gives me heartburn (I have a large hiatal hernia with spontaneous reflux, even in the standing position and Barrett’s esophagus on top of that, so you would think plain water would feel soothing going down). So I have had this habit for years to drink flavored seltzer because that agrees perfectly with me.
Every so often I puzzle about what the flavors might actually be. Essences, the term used on the labels, doesn’t explain at all what’s in my favorite Mandarin Polar seltzer.
The FDA states “natural flavors in sparkling water can be created using natural ingredients from essential oils, extracts, distillates or other products derived from fruits, vegetables, spices, herbs, barks, roots, and other organic substances.'” The Wall Street Journal’s research showed that the ‘essence’ in any given flavored seltzer is the same natural chemical used in other products, such as shampoo or ice pops. Taking the skin of a fruit, for example, and heating it to produce vapors that are then infused into the beverage.
Most companies are tight-lipped about their processing techniques. LaCroix’s website says “the flavors are derived from the natural essence oil extracted from the fruit named on our can – no sugars or artificial ingredients contained in or added to these extracted flavors.” However, some seltzer producers, like Spindrift, use alternative methods that actually use real fruit juice. Sip Trend claims that different flavors, other than the ones actually named, are occasionally used: a lemon-flavored seltzer might actually be infused with limes or even vegetables.
PFAS, short for per- and poly-fluoroalkyl substances, are chemicals designed to withstand water, oil, grease, and heat, which may sound ideal for food packaging. Until you learn that these chemicals take at least a century to break down in the human body, and much longer in our environment, and like many man-made substances approved for extensive use, they’re much less safe than we thought.
Linked to cancer, autoimmune disease, thyroid problems, and more health issues, PFAS’ toxicity is worrying, and still being studied. And unfortunately, PFAS are prevalent throughout our environment, from the seafood we eat to the water we drink.
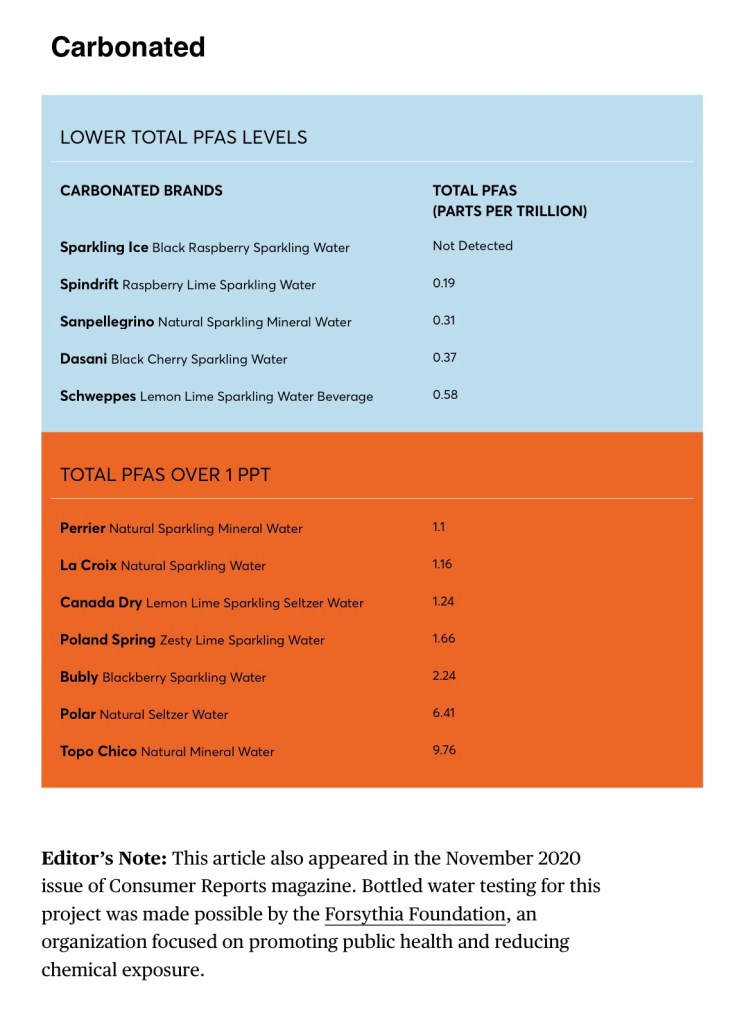
The federal government has issued only voluntary guidance for PFAS, saying the combined amounts for two specific PFAS compounds should be below 70 parts per trillion. A few states have set lower limits, of 12 to 20 ppt, according to American Water Works, an industry group. The International Bottled Water Association, another group, says that it supports federal limits for PFAS and that bottled water should have PFAS levels below 5 ppt for any single compound and 10 ppt for more than one. Some experts say the cutoff for total PFAS levels should be even lower, 1 ppt.
And in this Consumer Reports piece I found the number I was looking for: My favorite seltzer has the next highest forever chemical content of all tested seltzers.
My latest research has indicated that Schweppes club soda, which I like the taste of, has a PFAS level below 1 ppt, so I guess that will be my thirst quencher this summer.
My news sources (you can’t just say “the news” anymore, since everyone can choose what angle/bias/viewpoint/political spin they want to believe) are predicting that AI will very quickly replace midlevel professionals. Even in healthcare, areas like radiology seem to be pretty vulnerable to the advancing non-human capabilities.
In my practice I see many elderly people who are unable to use technology to interact with professionals outside their own homes. House calls are appreciated by patients and caregivers and give me as a physician a clearer picture of what my patients lives are like. And I hear every day how people have qualified for in-home help but the agencies don’t have enough staff to provide it. So I believe home health nurses and home health aides can feel fairly secure for quite a while.
And even if a doctor sees a patient in an office setting, getting a clear medical history is something not easily automated because of the way older people communicate and describe things. And when it comes to communicating a diagnosis and treatment options while also exploring each patient’s ultimate life goals seems nearly impossible to entrust to AI in my view. And the more diagnoses a patient has, the more judgment calls need to be made about where to set the priority, because what the patient primarily wants may not be exactly what the treatment algorithms would suggest.
There are many interesting examples in the literature of how two different doctors can prescribe the same medication and get totally different outcomes. This boils down to the personality and style of the doctor. Maybe you could teach AI what usually works, but patients need to see the face and know the name of their provider and it would be dishonest and immoral to make up fake names for AI “doctors“ communicating with patients.
As a side issue, liability in medicine has been a big concern, and I just read in my newsfeed today that in some places manufacturers of driverless cars will be held liable for traffic violations and presumably personal injury cases. I don’t believe the issue of liability with AI involvement in patient care is anywhere near settled.
When I look at my WordPress blog stats I often see what people call evergreen posts popping up, pieces that always seem to find relevance. But after work this afternoon I saw a title I almost didn’t recognize. It turned out to be from 2019 and it brought me back to a time of change in my life. But it also reminded me of how a lot of things have gotten tougher in life lately in so many more ways than just what I wrote about almost seven years ago:
I just realized none of the posts show on an iPad or a computer, but they do show on an iPhone. WordPress is working on this. In the meantime, please visit my Substack.
Osler said “Listen to your patient, he is telling you the diagnosis”. Duvefelt says “Listen to your patient, he is telling you what kind of doctor he needs you to be”.













{kind=link}